Thursday, December 30, 2021
Monday, December 27, 2021
Friday, December 17, 2021
Mysterious Wheat Penny

I noticed a coin on the kitchen floor yesterday. For some reason, I knew just looking at it that it was a wheat penny.
This design is out of circulation these days so it's unlikely that one would find them in change. They're not extremely valuable. Just an interesting coin. I like to keep them when I happen upon one.
But how did this wheat penny find its way to the floor in the kitchen? No one but me has been in there, probably for a month. I would have noticed it before it had been on the floor very long. It isn't one of mine because I keep them squirreled away in a change purse that I don't use.
I'm happy to have another wheat penny, even with a curious history. It's a 1946 coin, with an S under the date. I think that means the San Fransisco mint. Keep this and you'll never go broke!

Wednesday, November 24, 2021
Explosion of a Pyrex Measuring Cup

I was washing the dishes and put a Pyrex measuring cup in the cabinet. Yes, it clinked a little on the cabinet. KABOOOOOM!!! It didn't just break. It exploded into a zillion little needle like shards, flying all over the room. My Pyrex measuring cup, blown to smithereens. This was weird. In my fingers was the only remains, part of the handle. It was surprising that it didn't cause an injury.
I told my mother about it, and she seemed to be aware of the strange Pyrex dish reputation for explosions. "Tempered glass is under pressure, so that when it breaks it can explode," she informed me. Oh really? This was news.
As some may know, since I suppose I've raved about it, I've been something of a fan of my Duralex glasses. And so, hearing about the Duralex receivership, I visited the Amazon Duralex page to see if there were any of my wonderful glasses left. Goodness, I had a disturbing realization. First I read reviews that people had ordered bowls that spontaneously exploded in their hands without provocation. It sounded like the Pyrex measuring cup phenomenon. Well, maybe it was something about the shape of the bowls that just didn't work, I thought.
But then ... I read that glasses were also exploding ... tempered glass glasses. What?? I did have one glass that broke. I didn't see it happen, but I heard that it at least had the decency to break into a few pieces instead of millions of little needles. But these reviews were saying that the glasses exploded into dust. They were dangerous, they said.
I honestly don't know what to think now. I googled "exploding Pyrex," and there was an article by Consumer Reports that if the dish was taken to temperature extremes suddenly it might have a failure. This wasn't what happened to me. The merest touch and this measuring cup was history. No thermal extremes. Not even a clink that would have broken most dishes. It was an amazing sight to behold.
Go figure.
https://www.consumerreports.org/consumerist/why-pyrex-bowls-explode/
Soda-lime glass:
Borosilicate glass:
https://en.wikipedia.org/wiki/Borosilicate_glass
More Pyrex mayhem:
https://lajollamom.com/pyrex-glassware-explodes/
https://www.nbcmiami.com/news/local/pyrex-under-fire-for-reported-explosions/5939/
https://gizmodo.com/the-pyrex-glass-controversy-that-just-wont-die-1833040962
Friday, September 17, 2021
Dr. Alan Green MD's Anti-Aging Series
Dr. Alan Green. Episodes 1 - 8
https://www.youtube.com/watch?v=h4_zkfFV3aI&list=PLkfzM7KJv6vZ3rdGVMHIN2cM4i4aJ9lBB
My Road to Practicing Anti-Aging Medicine. Episode 1
https://www.youtube.com/watch?v=h4_zkfFV3aI&t=377s
My Theory of Aging. Episode 2
https://www.youtube.com/watch?v=Ts72rIBVbBk
Application of Senolytics in My Practice. Episode 3
https://www.youtube.com/watch?v=h3uG7ePEirY&t=329s
Rapamycin: Practical Dosage and Benefits. Episode 4
https://www.youtube.com/watch?v=3vszZEifmrA
The Importance of Maintaining Glutathione As We Age. Episode 5
https://www.youtube.com/watch?v=j86oA_5D1lE
My Longevity Protocol. Episode 6
https://www.youtube.com/watch?v=1JsuBS7ollQ
The Future of Aging. Episode 7
https://www.youtube.com/watch?v=ASqHeeBXkzw
Rapamycin for Longevity in Clinical Practice
Thursday, September 16, 2021
Saturday, August 14, 2021
Friday, August 13, 2021
Rapamycin and Antiaging - Is There Balm in Gilead?
"How much is Rapamycin worth? In my opinion, one million dollars a year." - Dr. Alan S. Green


Senescent Cells and Aging
Aging kills by age-related disease. Aging and age related disease are merely different manifestations of the same disease process. If not for aging; there would not be age-related disease.
At the center of Aging is elevated mTOR and senescent cells.
The purpose of this new website is to provide an in depth examination of the part played by senescent cells in Aging and age-related disease. The website also undertakes a detailed examination of senolytics, which are drugs which remove senescent cells.
There is now a sufficient body of evidence to justify the introduction of SENOLYTICS into clinical medicine.
https://senolyticstreatment.com/
Abstract
COVID-19 is not deadly early in life, but mortality increases exponentially with age, which is the strongest predictor of mortality. Mortality is higher in men than in women, because men age faster, and it is especially high in patients with age-related diseases, such as diabetes and hypertension, because these diseases are manifestations of aging and a measure of biological age. At its deepest level, aging (a program-like continuation of developmental growth) is driven by inappropriately high cellular functioning. The hyperfunction theory of quasi-programmed aging explains why COVID-19 vulnerability (lethality) is an age-dependent syndrome, linking it to other age-related diseases. It also explains inflammaging and immunosenescence, hyperinflammation, hyperthrombosis, and cytokine storms, all of which are associated with COVID-19 vulnerability. Anti-aging interventions, such as rapamycin, may slow aging and age-related diseases, potentially decreasing COVID-19 vulnerability.

Rapamycin Prolongs Life Span
From Mikhail Blagosklonny:
The three major criteria for potential anti-aging drugs are:
- A drug that prolongs life span in model organisms preferably mammals.
- A drug that prevents or delays several age-related diseases in mammals.
- A drug that suppresses cellular geroconversion from quiescence to senescent. [This statement means suppresses the formation of senescent cells. [3]
These criteria overlap each other. If an intervention extends life span, it must delay age-related diseases. Animals die from age-related diseases. For example, caloric restriction (CR) delays all diseases of aging and extends life span. One may say that CR extends life span by delaying disease. One may say that CR delays diseases by slowing down aging, Both interpretations are correct. CR deactivates the nutrient-sensing pathway, know as TOR (Target of Rapamycin). [2]
Rapamycin is essentially CR in a pill. They each target the exact same pathway, TOR.
Of all the known chemical substances in the universe, a Rapamycin has emerged as the most robust in extending lifespan. Rapamycin has extended the lifespan of every living thing tested in the laboratory: yeast, worms, flies, and even middle-aged mice. In a recent 2014 paper, it was reported rapamycin extended the median lifespan 23% in male mice and 26% in female mice.
From Matt Kaeberlein: "The drug rapamycin is currently the most effective and reproducible pharmacological approach for directly targeting the aging process to increase life span and health span in laboratory animals. Rapamycin positively impacts most hallmarks of aging and it has been shown to increase lifespan in each major invertebrate model organism and in rodents. Rapamycin increases life span by 10 to 30% in multiple strains of mice." [4]
Blagosklonny and Kaeberlein are the two foremost experts on the theory and practice of rapamycin.
3. Blagosklonny, From rapalogs to anti-aging formula, Oncotarget. 2017 May 30; 8(22): 35492–35507.
4. Kaeberlein, Rapamycin and Alzheimer's disease: Time for a clinical trial?, Sci Transl Med. 2019 Jan 23;11(476).
Rapamycin Prevents Age-Related Disease
From Blagosklonny: "Rapalogs prevent age-related diseases in mice as well as in other mammals including non-human primates and humans. As examples: rapamycin prevents atherosclerosis, neurodegeneration and retinopathy and cardiomyopathy in rodents. Rapalogs prevent cancer in mice and humans. Rapamycin decreases obesity in mice and humans. As predicted, rapalogs rejuvenate immunity, improve immune response in mice and humans." [3]
From Kaeberlein: "Not only does rapamycin treatment increase life span but it also delays, or even reverses, nearly every age-related disease or decline in function in which tested in mice, rats and companion dogs, including cancer, cardiac dysfunction, kidney disease, obesity, cognitive decline, peridontal disease, macular degeneration, muscle loss, stem cell function, and immune senescence" [4]
The above statements regarding Life span extension and prevention of age-related disease might seem fanciful, overimaginative and unrealistic. However, the quotes come from a 2017 and a 2019 paper prepared by the worlds leading authorities. Furthermore, a review of these two papers will show multiple references to support and document each and every statement.
Not mentioned in above was a very large body of evidence that rapamycin is the leading drug to prevent Alzheimer's disease. Alzheimer's disease is discussed in following section.
Rapamycin also prevents insulin resistance, metabolic syndrome, osteoarthritis, osteoporosis and age related chronic lung disease.
Rapamycin Slows Formation of Senescent Cells
Criteria (3) above for potential anti-aging drug was suppressing formation of senescent cells.
In a 2018 paper Blagosklonny states, "It has been calculated than rapamycin slows geroconversion by approximately 3-fold". This means rapamycin slows formation of senescent cells three-fold. [5]
The Blagosklony theory of aging is that aging is hyperfunctional.
From Blagosklonny: "Killing senescent cells is beneficial because senescent cells are hyperfunctional. The hypersecretory phenotype or Senescence-Associated Secretory Pheontype (SASP) is the best known example of universal hyperfunction. Most hyperfunctions are tissue-specific. For example, senescent beta cells overproduce insulin and this activate TOR in hepatocytes, adipocytes, and other cells, causing their hyperfunction, which in turn leads to metabolic syndrome (obesity, hypertension, hyperlidemia, and hyperglycemia) and is also a risk factor for cancer. SASP, hyperinsulinemia, obesity, hypertension, hyperlipidemia and hyperglycemia are all examples of absolute hyperfunction (an increase in functionality)." [6]
"Killing senescent cells is beneficial because senescent cells are hyperfunctional." [6]
"Senolytics are drugs that extend life span and delay some age-related diseases by killing senescent cells. Targeting senescent cells have been shown in animal models to prevent age-related pathologies such as emphysema, lung fibrosis, atherosclerosis, osteoporosis, osteoarthritis, renal disease, intervetebral disc pathology, hepatic steatosis (fatty liver) and other age-related conditions." [6]
The above list of age-related disease shows why preventing the formation of senescent cells is so important. Senescent cells are extremely harmful and the harm causes by senescent cells can be lowered by preventing their formation in the first place (rapamycin) or killing senescent cells by drugs called senolytics.
These three sections show how rapamycin fulfills the criteria for potential anti-aging drugs.
Nothing in the entire universe of drugs comes close to rapamycin and other rapalogs in fulfilling these three criteria of potential anti-aging drugs.
5. Blagosklonny, Does rapamycin slow down time?, Oncotarget. 2018 Jul 13; 9(54): 30210–30212.
6. Blagosklonny, Paradoxes of senolytics,. Aging (Albany NY). 2018 Dec; 10(12): 4289–4293.
Aging is easily treatable
A recent paper by Blagosklonny has the provocative title: "Disease or not, aging is easily treatable". The first sentence is: "For decades, one of the most debated questions in gerontology was whether aging is a disease or the norm."(7)
In my opinion, this entire debate is obsolete, archaic and medieval. Galen, a philosopher in ancient Greece put forth the idea that aging was not a disease, because everybody got aging and therefore aging was natural. Galen also originated the miasma theory which held that diseases such as cholera and epidemics like the Black Death were due to "bad air." In the second half of 19th century the germ theory of infectious disease exploded Galen's miasma theory. It is also time for Galen's theory of aging to be consigned to the "ash heap of history"
The answer provided by Blagosklonny is: "It does not matter because aging is already treated using a combination of several clinically-available drugs, including rapamycin...For treatment purposes, aging is a deadly disease (or more generally, predisease), despite being a normal continuation of normal organismal growth. It must and, importantly, can be successfully treated thereby delaying classic age-related diseases such as cancer, cardiovascular and metabolic diseases, and neurodegeneration." (7)
In my practice, I have treated over 380 patients (Oct 2019) and the one question nobody ever asked was whether aging was a disease or was natural.
Aging should be considered a "term of art". In my practice aging can have TWO meanings:
A. "Aging is the sum of all age-related disease." This means aging is the sum of pre-disease and clinical disease.
B. Aging is also used as being short for TOR-driven aging as in the title: "TOR -driven aging, Speeding car without brakes" (Blagosklonny, 2009 [2]
Aging mechanisms which is not TOR-driven aging is put in category "post aging syndrome.
Aging must be connected to pre-disease or clinical disease. Aging is not an abstract concept. Aging is pathology.
"In pre-disease, abnormalities have not reached the arbitrary diagnostic criteria of the disease. So, aging consists of progression from (pre)-pre-disease (early aging) to disease (late aging associated with functional decline). Aging is NOT a risk factor for these diseases, as aging consists of these diseases: aging and disease are inseparable. [7]
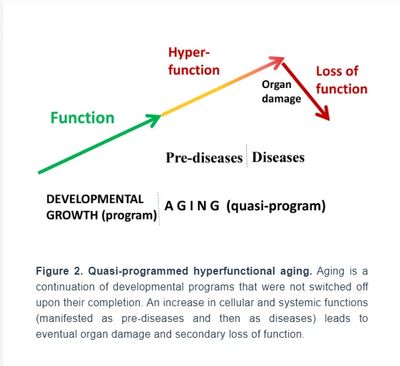
In this paper, Blagosklonny has a very instructive diagram: GROWTH-->AGING. Initially aging is Hyper-functions in the pre-pre-disease and the Pre-disease stages, then aging ends in loss of function and Death.
Caption: Relationship between aging and disease, "When growth is completed. growth-promoting pathways increase cellular and systemic functions and thus drive aging. This is a pre-pre-disease stage, slowly progressing to a pre-disease stage. Eventually, alterations reach clinical disease definitions, associated with organ damage, loss of function (functional decline), rapid deterioration and death."
NORMATIVE AGING
The concept of "normative aging" is where the Blagosklonny concept of aging splits entirely from conventionally thinking. In conventional thinking normative changes, that which is the norm, is not a disease at all. In the Blagosklonny concept of aging, NORMATIVE AGING is the quintessential disease of aging. Unrelated humans share 99.5% genetic similarity. Therefore, it makes complete sense that something as fundamental as TOR-driven aging should effect everybody. Those changes that effect everybody are the bed rock of the disease. In an extremely important paper discussed below under the topic of normative brain aging; it was shown that rapamycin prevents deterioration of cognitive and vascular decline in the aging rat brain. That paper is the complete vindication of the concept of TOR-driven aging and prevention of pre-disease.
Healthspan. This term refers to the subclinical disease period. "In theory, a treatment that slows aging increases both healthspan (subclinical period) and lifespan. The goal of both anti-aging therapies and preventive medicine is to extend healthspan (by preventing disease), and thus extending total lifespan.
Preventive Medicine vs Anti-aging medicine
The goal of preventive medicine is to present disease by treating pre-disease. This is the same goal as anti-aging medicine. The difference between classic preventive medicine and anti-aging medicine is the cornerstone of anti-aging medicine is slowing aging.
When you start with preventive medicine and add rapamycin to slow aging, you have transformed preventive medicine into anti-aging medicine.
Conclusion: "Anti-aging drugs such as rapamycin delay age-relate diseases. In order to extend life span, an anti-aging drug must delay age-related disease...
"And this approach is actually being used now to treat aging at Alan Green's clinic in Little Neck, NY."(7)
7. Blagosklonny, Disease or not, aging is easily treatable, Aging (Albany NY). 2018 Nov; 10(11): 3067–3078..
Epigenetic Clock Shows Rapamycin Slows Aging
Recent paper by Steve Horvath shows rapamycin suppresses the progression of aging as shown by the Horvath epigenetic clock. (8)
The Horvath clock is a major achievement in aging research. The Horvath DNA methylation epigenetic clock is an objective way to measure biologic age independently of time.
In this study Horvath showed that rapamycin reduced biologic aging of growing skin cells in culture. Rapamycin is now the first drug and so far the only drug shown to slow epigenetic aging.
Rapamycin reduced cellular proliferation rate, reduced somatic cell differentiation, REDUCED NUMBER OF SENESCENT CELLS and preserved proliferative capacity, however these specific effects were separate and distinct from slowing of the epigenetic clock.
The paper concluded: "In summary, the observations above represent the first biologic connection between epigenetic ageing and rapamycin.
These results for human cells add to the evidence that extension of life, at least by rapamycin, is indeed accompanied by retardation of ageing.
These observations also suggest that the life-extending property of rapamycin may be a resultant of its multiple actions which include, but not necessarily limited to SUPPRESSION OF CELLULAR SENESCENCE AND EPIGENETIC AGING, WITH THE POSSIBILITY OF AUGMENTATION OF CELLULAR PROLIFERATION POTENTIAL." [8]
This paper is huge. Prior to this paper the evidence that Rapamycin slows aging was the indirect evidence of extension of mouse and other lifespans.
This study is direct evidence on human cells of rapamycin slowing aging.
8. Horvath. Rapamycin retards epigenetic ageing of keratinocyts independently of its effects on replicative senescence, proliferation and differentiation, Aging (Albany NY). 2019 May 31; 11(10): 3238–3249.
Rapamycin/TOR Anti-aging Medicine
TOR has two components, TOR1 and TOR2. Rapamycin has only one action, it blocks TOR. TOR1 is very sensitive to a single dose of rapamycin and TOR2 is very resistant. Therefore, intermittent use as weekly rapamycin can be used to block TOR1 and not block TOR2.
Rapamycin anti-aging preventive medicine is a combination of Anti-aging Medicine and Preventive Medicine as regards prevention of age-related disease.
Both seek to prevent disease and thus extend health span and prolong life span. Both treat pre-disease to prevent clinical disease. The difference is Preventive medicine uses classic methods to prevent specific age-related diseases. Anti-aging medicine seeks to slow down aging and thus delay all age-related disease. The cornerstone of slowing aging that this office uses is rapamycin. The target is TOR1. The basic concept is TOR1 is driving age-related disease.
The special expertise of this office is knowing how to use rapamycin to lower TOR1; but not lower TOR2
There are no published studies on how to use rapamycin to lower TOR1 and not TOR2 and get a satisfactory result. Knowing how to properly use rapamycin as an anti-aging drug is based upon experience and the art of medicine.
At this time (Sept 2019), the office has been treating patients with intermittent rapamycin for over 2 1/2 years and has treated over 350 patients. I have also taken rapamycin myself for close to 4 years.
The medical literature lists many side-effects from use of rapamycin. Many experts say that rapamycin has too many side-effects to be used for anti-aging medicine. It is true that rapamycin is a potent prescription drug and as is true for all prescription drugs; people who do not know what they are doing should not use or prescribe them. Rapamycin is not for the uninitiated or for those health care providers who lack sufficient expertise required to use rapamycin in a knowing manner.
COME FOR THE FUTURE, STAY FOR THE PRESENT
The ever expanding evidence in the scientific literature is that rapamycin slows aging, extends life span and delays and decreases risk of a large number of age-related diseases.
What is not clear from the literature is the effect in the present, not the future. Ameliorating pre-pre disease and pre-disease can have a dramatic impact on quality of life in three to six month from onset of treatment. One of most noticeable effects is on the brain. Overall mood and feeling of well-being is frequently improved.
- Many patients report their brain is sharper, functions better, and processes information better.
- Cardiac symptoms of fatigue and shortness of breath with exercise may be significantly improved. This is especially evident if hike or jog or walking up hills.
- Muscles stay strong.
- Skin looks younger.
- Rapamycin is also the premier weight loss drug. One can get back to the waist size one had when they were twenty-something.
- Chronic kidney disease improves. Stage 3 chronic kidney disease, as measured by GFR (glomerular filtration rate) can improve to stage 2 and stage 2 to normal.
- Mild osteoarthritis can improve.
- Prostate lower urinary tract symptoms such as urgency, frequency and nocturia are frequently improved.
Rapamycin treatment is not about waiting till you are 100 years old and noting all the diseases you dodged; or about a clinical study that follows people for 10 years and does calculations about "Odds ratio" [OR].
For many of my patients, slowing aging is about feeling better now [in the present] with life span extension and disease prevention something in the distant future rapamycin provides to boot.
However, not all patients have pre-clinical disease. Many have serious disease in the present.
In basic science, rapamycin has emerged as the silver bullet for the treatment of a large number of age-related diseases. However, rapamycin is a generic drug. In the United States, we are not Communists and nobody is expected to spend millions of dollars on clinical studies for which they can not receive any monetary benefit. Therefore, no human clinical studies are anticipated for rapamycin. However, the basic science research suggests that rapamycin is the greatest new drug to emerge since Penicillin, some ninety years ago. This office seeks to accommodate those persons who seek protection from age-related disease in their own lifetime. For this purpose, this office relies heavily upon animal models and basic research.. The premise underlying treatment is that those of us who need geroprotection now, would most likely be dead before appropriate clinical trials are initiated, completed, evaluated and the results incorporated into clinical practice.
This office practices Rapamycin Medicine. Rapamycin Medicine is the application of the theory and research of Mikhail Blagosklonny to clinical medicine. The Blagosklonny theory of aging and age-related disease is presented below in the following section, Blagosklonny Literature. In short, the theory is elevated TOR causes TOR driven aging and TOR driven aging causes age-related disease. Age-related disease and death is a late manifestation of the damage caused on a cellular and molecular level by elevated TOR.
Rapamycin Medicine is the "off-label" use of rapamycin for prevention and amelioration of these diseases.
This website attempts to present a very large amount of science-based information based upon quoted scientific papers. Almost all papers quoted are "open-label" and readers are encouraged to download and study all references.
CAVEAT: While I have been on weekly rapamycin for close to 4 years and I am very pleased with the results, and Mikhail Blagosklonny predicts rapamycin will become the standard of care in our lifetime for anti-aging protection; nevertheless, to the best of my knowledge, NO OTHER PHYSICIAN IN THE UNITED STATES HAS A SIMILAR PRACTICE USING WEEKLY RAPAMYCIN AS THE CORNERSTONE OF AN ANTI-AGING/ PREVENTIVE MEDICINE PROGRAM as regards age-related disease. Furthermore, the majority of physicians do not believe there is a common underlying cause for diseases of aging or that lowering TOR can prevent such disease.
Use of weekly Rapamycin as the cornerstone of an anti-aging formula has not been proven by human clinical trials. Such treatment is not recognized by the FDA. There is not the safety of many physicians having used a similar weekly rapamycin treatment for many years.
Consequently, a careful analysis is necessary to make a proper informed decision regarding use of weekly rapamycin.
Disease A:
- Cancer
- Atherosclerotic heart Disease
- Age-associated Cardiomyopathy
- Obesity
- Fatty Liver Disease (NAFLD)
- Osteoarthritis
- Diabetes type 2, Insulin resistance
- Hypertension
- Hearing Loss
Disease B:
- BPH (Benign prostatic hyperplasia)
- Osteoporosis
- Age-related Macular degeneration
- COPD (Chronic lung disease)
- Chronic renal disease
Neurodegeneration:
- Alzheimer's disease (Prevention)
- Parkinson's disease
- Tauopathy
In the drop-down section the evidence is primarily from basic science and animal studies.
Disease A has more evidence and studies than Disease B
APOE4 carriers should consult linked website Alzheimer-prevention.com

Rapamycin
In "Koschei the Immortal and Anti-aging Drugs", 2014, Blogosklonny, sets forth an anti-aging formula. Rapamycin is the cornerstone of that formula. Rapamycin was approved in 2009 for use in transplant medicine. For that purpose it has been used in over a million people with good results with foreign organ retention for many years. Rapamycin is generally well tolerated with only mild to moderate side-effects. I stipulate that the dose and manner of use of Rapamycin in transplant medicine is hazardous to your health and certainly that manner of use is in no way suitable for anti-aging medicine.
In transplant medicine they start with somebody with a normal level of mTOR function and use rapamycin to knock mTOR activity down to almost zero level of activity. Then they keep mTOR at this very low level. The goal is to totally disrupt normal mTOR function and signaling. This complete disruption of normal mTOR function causes a severe disruption of lymphocyte function. The net result is you can put a foreign organ into a person and not get an immediate violent rejection and infarction of the transplanted organ. This is how the body is supposed to react. However, as long as mTOR is kept continuously depressed, the immune system will not function properly and orchestrate rejection of the foreign organ. This is great medicine and saves lives. The extraordinary thing is the "experts" who ascribe the same side-effects seen in transplant medicine to the effects they claim would be seen if rapamycin was used in anti-aging medicine.
It was well known in medicine 500 years ago that whether a drug is poison or safe is a matter of dose. Indeed, consuming 4 liters of water quickly is fatal 50% of time [LD 50] due to sudden hyponatremia and brain swelling and edema. Nobody says water is too dangerous to drink.
In anti-aging medicine, Blagosklonny recommends intermittent or pulse treatment and also suggested weakly dosage.Rapamycin has a half-life of @ 62 hours. That means daily use is once every 0.4 half-lives while weekly use is once every 2.7 half lives. For that reason, only data regarding using rapamycin once a week is applicable to side-effects expected from once a week use and side-effects from daily use are not applicable.
In my practice, I consider the proper anti-aging dose of rapamycin to be 2-6 mg, and the proper interval 1-3 weeks. So the most conservative anti-aging dose would be 2 mg once every 3 weeks.
I would certainly welcome formal research studies on the best dose and best interval and I expect to see those results in about 50 years from now.
Caloric Restriction
Caloric restriction is major component of Koschei formula. Caloric restriction has been known to extend life span in numerous species from worms to mice for 100 years. Caloric restriction prevents age-related diseases including cancer and atherosclerotic heart disease. Interestingly, caloric restriction ameliorates sarcopenia. While caloric restriction increases insulin sensitivity, severe caloric restriction produces a glucose intolerance picture which is benign in significance. A 2015 study in mice showed mechanism of action of caloric restriction was inhibition or TOR and increase in SIRT1. Thus caloric restriction is different from rapamycin alone which only inhibits TOR.
In a very important study in humans, there was 25% caloric restriction in one group and 12.5% caloric restriction in another group combined with 12.5% increase in energy use through exercise. Compared to control group the caloric restriction group and the caloric restriction group plus exercise had similar results. There was a 20 pound weight loss, mostly body fat. Fasting glucose remained about the same; but fasting insulin levels went down 33%. Adiponectin showed 17% increase. SIRT1 level increase 3 fold. There was indication of decease in oxygen free radicals in muscle by 22%. Most important was the effect on mitochondria. Mitochondria increased in number and became more efficient. The increased efficiency of mitochondria was shown by reduced basal energy use at rest and less production of free radicals.
The best natural experiment showing what caloric restriction can do to a human population is the traditional Okinawan diet in the years 1950 to 1995. These people were farmers who worked very hard and as a matter of culture consumed less food. Studies calculated that they took in 8% less calories than their requirements. They had a remarkable decrease in age-related disease. Compared with Americans, men had 17% incidence of coronary heart disease and women 8%. Men had 50% incidence of colon cancer and women 30%. Men had 14% incidence of prostate cancer and women 9% incidence of breast cancer. As regards average life span, it was 5 years longer than Americans. The oldest 1% lived to 105 compared to 101 for oldest 1% of Americans. For the last 20 years, Okinawans have switched to a more traditional Japanese caloric intake and they no longer show any health benefits.
The Okinawan experience shows that an 8% caloric restriction less than required can achieve excellent results.
Most people notice that after a period of time on a caloric restriction diet they stop losing weight. They then get discouraged and go off the diet. In the Koschei formula, the purpose of a diet is not to lose weight; but rather maintain weight on less calories. It is not the weight loss; but the caloric restriction itself which results in the health benefits.
Physical Activity
Physical activity is a very important part of the Koschei formula. Blagosklonny states, "chronic physical exercise inhibits mTOR and increases insulin sensitivity."
For an excellent study on the cellular mechanisms and signaling pathways through which physical activity decreases insulin resistance, see 2008 paper by Erin Glynn entitled, "A chronic increase in physical activity inhibits the fed-state mTOR/S6K1 signaling and reduced IRS-1 serine phosphorylation in rat skeletal muscle." The very short explanation is physical activity causes activation of AMPK energy sensing pathway, which leads to a decrease in insulin resistance in skeletal muscle. Muscle is the major regulator of insulin resistance as skeletal muscle is responsible for up to 75% of insulin dependent glucose disposal in humans.
In the book, "Autobiography of Geronimo", it was stated that Apaches could travel 70 miles a day on foot. There are ultra-marathon runners who train for runs of 50-100 miles. If they ever see a doctor, it is about running related injuries as they have very low level of age-related disease. The major negative effect of civilization on human health is that civilization caused a decrease use of leg muscles. Humans are by nature, the greatest long-distance runners of the animal world.
The question is: "what is the minimum level of physical activity needed"? The minimum requirement seems to be burning 1000 calories a week; the equivalent to walking 10 miles. One study showed that moderate physical activity is associated with 50% reduction in cardiovascular disease in over-65s. Another study had shown that moderate physical activity of walking 4 hours a week had a 54% reduction in cardiovascular mortality and a high level which was described as jogging 3 hours a week, had a 66% reduction.Note that the difference between moderate and high was small; but the difference between moderate and low activity was dramatic.The conclusion of the study was that older adults who are physically active have a lower risk of coronary heart disease, stroke, and death from cardiovascular disease.
The main point is that physical activity, like walking or jogging, causes a decrease in insulin resistance in leg muscles. A decrease in insulin resistance causes a decrease in insulin levels which causes a decrease in mTOR.
Metformin
Metformin is part of our anti-aging formula. In a 2014 UK paper metformin monotherapy had a 15% longer survival than non-diabetic control subjects. Survival of diabetic patients not on Metformin had a survival 23% lower than non-diabetic subjects, which reflects expected results.
In a NIA (National Institute of Aging) 2016 study, metformin used alone had a modest increase in life spanbut only in male mice.When metformin was combined with rapamycin there was a very dramatic increase in one of two strains of mice. Male and female mice had a 24% increase in median life span and 10% and 17% increase in maximum life span. This was an impressive increase over rapamycin alone.
Metformin has been shown to reduce cancer in a great majority of animal studies and many human studies, especially liver and pancreas. Metformin acts through very interesting pathways which include activation of LKB1 (a tumor suppressor) and then stimulation of AMPK pathway which inhibits TOR.
For such an excellent drug, the question is why Metformin doesn't get more attention. A leading researcher on Metformin, explained, "The problem with Metformin is it's cheap, it's widely available, it has a great safety profile, and anyone can use it."
Metformin is also excellent to combine with rapamycin as the two agents have many opposite side effects, which can cancel each other's negative side effects.
Angiotensin II disruption
Angiotensin II disruption is an extremely important part of the anti-aging formula. In clinical medicine today, there are two ways to disrupt angiotensin II, angiotensin-converting enzyme inhibitors (ACEIs, [Lisinopril, enalapril] and angiotensin II receptor blackers (ARBs, (Losartan, Candesartan). [We only use those that cross the blood-brain barrier]. These drugs are the most popular drugs used for the therapy for hypertension and are used by millions for that purpose. However, angiotensin II is involved in far more than just hypertension.
Two great parallel systems on the cellular level are the TOR system and the angiotensin system. The TOR system is 2 billion years old and the angiotensin system is 500 million years old. The evolution of the angiotensin system was essential for the development of a circulatory system, which was required for animals to get bigger than a few millimeters, the distance for effective diffusion.
There are two main theories of aging. The hyperactive TOR theory first presented in 2006, and the ROS theory (reactive oxygen species) first presented in 1956. The hyperactive TOR theory is about early aging and diseases of aging related to hyperactive TOR, and the ROS theory relates more to late aging. [see first section Blagosklonny Medicine] The current major focus of the ROS theory is on mitochondria, the major source of oxygen free radicals. Angiotensin is intimately involved with mitochondria and oxygen free radicals. While TOR is strictly organic chemistry, in the angiotensin system, the most important components are small molecules, superoxide and Nitric oxide.
Disruption of angiotensin II, prolongs lifespan of mammals. In hypertensive rats, treatment with angiotensin II inhibition with ACEIs or ARBs ameliorated the harmful vascular effects of hypertension and doubled the rats lifespan. In a study of normal rats without hypertension, Enalapril, an ACEi prolonged lifespan by 21.4% and Losartan, an ARB, increased lifespan 12.5%.
In an extremely important study by Begnigni, 2009, "Disruption of the Ang II type 1 receptor promotes longevity in mice", they created homozygous mice with knock-out of the Ang type 1 receptor. The knock-out mice lived a remarkable 26% longer than the controls. The knock-out mice showed protection from atherosclerosis and vascular damage. The knock-out mice also showed reduced age-induced mitochondrial loss. The conclusion was that reduction in oxidative stress ameliorated mitochondrial loss. They also showed an increase in genes for Nampt and SIRT3. Caloric restriction also has this effect, but not rapamycin, which only extends lifespan by inhibition of TOR. This study showed that knock-out Ang II receptor increased lifespan dramatically, but it seemed through a separate system than inhibition of TOR. Caloric restriction appears to have one foot in each system.
In a separate study of genes associated with extreme human longevity, Begnigni showed that genes with variations in angiotensin II receptor, which decreased function, were associated with extreme longevity.
Another study in humans showed treatment with angiotensin II inhibitors reduced risk of cancer, hazard ratio of 0.66.
For an understanding of the extraordinary roles of angiotensin II on age-related disease, I recommend reading, "Angiotensin II revisited: new roles in inflammation, immunology and aging", by Ariela Benigni, 2010. For the role of angiotensin II regarding mitochondria, I recommend "Renin-angiotensin system inhibitors protect against age-related changes in rat liver mitochondrial DNA content and gene expression", Elena de Cavanagh, 2008.
Aspirin and Statins
Aspirin is the only "anti-aging" drug recommended by the US Preventive Task force. The recommendation is for men 45-79 and women 55-79 to prevent cardiovascular disease and colorectal cancer. They did not specify 81 mg or 325 mg. I recommend 81 mg to decrease risk of upper gastrointestinal bleed.
I agree with evidence showing aspirin has a very beneficial effect on health of endothelial cells. The effect is mediated through both inhibition of platelets and decrease in chronic inflammation of endothelial cells. Part of the protective effect of Aspirin on endothelial cells is through blocking an inhibitor of NO synthase and increasing production of Nitric oxide. The increase in Nitric oxide causes a decrease in vasoconstriction and is similar to pathway of Ang II inhibitors who's main action is to increase Nitric Oxide.
I also agree with data that aspirin decreases risk of colon cancer.
One important study (Wan, 2013), established aspirin as a true anti-aging drug. The study was "Aspirin extends the lifespan of C.elegans via AMPK and DAF-16/FOXO in dietary restriction pathway." In this study aspirin was shown to activate LKB1. LKB1 is a very important tumor suppressor. LKBI then activates AMPK which in addition to many other beneficial effects also inhibits mTOR. This puts aspirin in same pathway as metformin with activation of LKB1 and AMPK. In contrast to Rapamycin, which has a single action; the direct inhibition of mTOR; Aspirin and Metformin are indirect inhibitors of mTOR and also involved in many other pathways.
Statins are included in our anti-aging formula. In addition to usual reasons for using statin; rapamycin can cause elevation of lipids. This elevation is a result of beneficial effect in that rapamycin prevents lipids from entering tissues and rapamycin has a robust anti-atherogenic effect regardless of elevated lipids. However, lowering serum lipids with statins through decreased production in liver is beneficial and synergistic with the rapamycin effect of removing lipids from atheroma.
In the 2013 Cochrane report, which reviewed 19 trials involving 60,000 patients with mean age 57, statins reduced all cause mortality (OR 0.86). In a VA study, all cause mortality was also decreased (OR 0.54) and the conclusion was "statins showed a highly significant negative association with death."